How the Taboo of FGM Became a Global Challenge
By Renée Bouhuijs and Magdalena Uerlich
“The body is not like a suit of clothes, to be hemmed and stitched to the style of the times.”
Dr. Paul McHugh, Johns Hopkins University

On November 11th 2014, the international conference on Female Genital Mutilation / Cutting (FGM/C) was held in Copenhagen. During this day, it became very clear that the issue of FGM/C is closely related to the health of many women, and importantly from a global health perspective, that it should be acted upon through a global movement and through stimulating community development in general. This comes in relation to the announcement of a global media campaign of the UN and The Guardian to end FGM/C within a generation.
UNICEF refers to FGM/C as “all procedures involving partial or total removal of the external female genitalia or other injury to the female genital organs for non-medical reasons”.
Four types of the practice can be distinguished:
Type 1: Excision of the prepuce, with or without excision of part or all of the clitoris.
Type 2: Excision of clitoris with partial or total excision of the labia minora.
Type 3: Excision of part or all of the external genitalia and stitching/narrowing of the vaginal opening (infibulation).
Type 4: Pricking, piercing or incising of the clitoris and/or labia. Stretching the clitoris and/or labia. Cauterization by burning of the clitoris and surrounding tissue. Scraping of tissue surrounding the vaginal orifice (anguriya cuts) or cutting of the vagina (gishiri cuts). Introduction of corrosive substances or herbs into the vagina to cause bleeding or for the purpose of tightening or narrowing it. Any other procedures that fall under the above definition.
The reasons for practicing FGM/C, however, are diverse. Some mention the control over women’s sexuality, where “FGM, in particular infibulation, is defended in this context as it is assumed to reduce a woman’s sexual desire and lessen temptations to have extramarital sex thereby preserving a girl’s virginity”, as well as hygiene, as uncut women are seen as dirty. Moreover, gender based factors are often mentioned. FGM might also be practiced as to enhance a girl’s femininity, which may be synonymous to docility and obedience. The link to religion is often made, although religious writings do not mention FGM/C.
Present situation
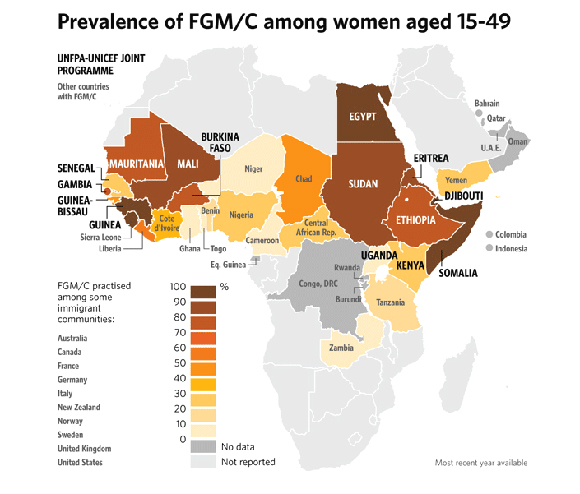
The estimated prevalence of women between the ages of 15 and 49, affected by FGM type 1, 2 or 3, is still extremely high in some African countries. Somalia has the highest estimated prevalence with 97.9 % (2006), followed by Guinea with 95.6% (2005) and Sierra Leone with 94% (2006).
In terms of globalisation related to health, we think it is interesting and relevant to address what will happen to prevalence rates and the situation in general if people start migrating and moreover, what the global response is to this issue which still affects millions of girls and women.

Looking at the European level, according to the European Commission, there is a lack of reliable and comparable data on the prevalence of FGM at EU level due to under-reporting and incompleteness. It is estimated, however, that hundreds of thousands of women living in Europe have been subjected to genital mutilation and thousands of girls are at risk. The largest groups of women and girls originating from countries in which the practice of FGM/C is widespread live in the following EU countries: Austria, Belgium, Denmark, Germany, Spain, Finland, France, Ireland, Italy, the Netherlands, Portugal, Sweden and the United Kingdom.
In relation to migration, changes can already be seen in the perspective towards FGM/C practices in the first generation of migrants. It is essential to realise that these changing perspectives are not merely an issue of a sudden change after migration; countries or areas of origin might have a history of campaigning against FGM/C. Transitioning to a new area or country may strengthen and encourage feelings that had been developed already. For instance, a study in Britain found that a majority of young Somali women who came to London at a young age, seemt to be uncut.
Risks of FGM/C are likely to get lower once people can withdraw from social pressure. However, some new fears may come in place such as that family members, in the home country, still want to circumcise daughters. Also, transitioning from cut to uncut generates new behaviour among girls, which might be a concern. Some of the EU countries have implemented laws to eliminate FGM practices, including making practices punishable even if conducted in another country.

Work being done to fight FGM/C
We are familiar with a number of initiatives that address the issue of FGM/C and, furthermore, during the international FGM/C conference it became clear what the current global movement to abandon these practices within one generation entails. In general, over the last few decades multiple campaigns have been developed to address the issue of FGM/C. The Orchid project, the Waris Dirie Foundation, UNICEF and Amnesty International are just a few organisations that work together with local NGOs on educating communities and lobbying for national laws against FGM. As Molly Melching of the organisation Tostan emphasised at the FGM/C conference, it is essential to regard the development of communities as a greater good, which will have its influence on abandoning FGM/C practices. With the development and strengthening of communities come the focus on governance, democracy and human rights. Merely educating communities will not be sufficient however, men need to get involved actively and might want to be used as role models in the process of abandoning FGM/C. This is what it takes to get a broader outreach, as pointed out by Jensen, the Danish minister for Trade and Development Cooperation during Copenhagen’s international FGM/C conference. Besides, as stressed by Nafissatou Diop (coordinator for the UNFPA/UNICEF joint programme on FGM/C), in order to stop the so called medicalisation of FGM/C – the execution of it in medical centres or clinics – it will be vital to work towards a better integration of prevention within health services and greater visibility of the communities that have succeeded in actually changing.
Remarkable in aforementioned discussion is the call for more pressure on the political environments of the countries that are greatly affected by FGM/C, while these countries were not represented at all during the international conference. This raises an essential point in tackling issues like FGM/C and one could argue that this is one of the aspects that should be considered most when discussing FGM/C practices.





Leave a comment