By Tara Pollak
Humans are mammals. Breasts, or mammae, are quintessentially human; most of us have them and some of us feed from them. But that is just it:
Some of us feed from them, and some don’t. Most people have breasts, but some don’t.
The insistence of public health initiatives to increase breastfeeding rates globally, and to support a return to “natural” nurturing practices is important. Yet, having spent a summer in Ireland interviewing breastfeeding women and community midwives, I want to offer some observations on what breastfeeding looks like in practice, and how to support it. In a review of interviews, and snippets of conversations, I contextualise the technicalities of “natural” breastfeeding and point to the socio-political and economic factors that stand in the way of any well- intended public health campaign.
First, a little bit about breastfeeding in Ireland.
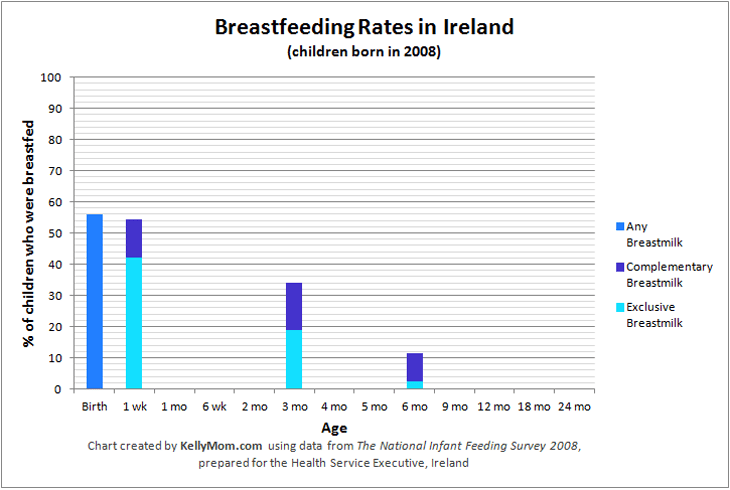
The Republic of Ireland has some of the lowest breastfeeding rates in Europe. The initiation rates are rising, with over half of all hospital birthing parents initiating breastfeeding. Parents try. At six months, the WHO recommended minimum duration for exclusive breastfeeding, only about 2.4% of Irish parents continue to breastfeed. Something occurring after the initial push, hospital release and after-care counteracts breastfeeding attempts.
Trying to uncover the motivations and struggles of breastfeeding parents in Ireland, I spent six weeks in County Cork and Dublin speaking to 18 women and mothers, as well as three community midwives. I have grown up with statistics and papers about the advantages of breast milk as my mother- ironically, works for a formula company. This project was an attempt to make sense of the small number of Irish breastfeeding parents through a historical, social and discourse analysis, rather than rely on hospital statistics alone. I established contact mainly through online breastfeeding forums and invited my informants for informal interviews. It is important to note that all my informants had children, were in a partnership, on maternity leave or employed and from a white middle-class background. Their education and economic stability is a decisive factor in their breastfeeding success, and the outcomes of this research project.
Irish public health initiatives attempt to make breastfeeding appealing using phrases like “[breastfeeding] is the ideal and complete form of nutrition”, and “breastfeeding is the norm for infants and young children in Ireland”. The science of breast milk is astonishing, and very convincing. Breastfeeding literature, which is circulated in ante-natal classes and easily accessible online does not explain however, how to breastfeed in practical examples. After an emergency Caesarean and surgical complications, Izzy was desperate when she found out that she had hardly any milk. The hospital forgot to forward her release to the public health nurse, and over the next two weeks, Izzy spent a lot of money calling Lactation consultants to help her. Building contraptions of tubes and pumps, Izzy managed to feed her infant. Is this a “natural” way of nurturing? Or a technical intervention in a desperate situation? Difficulties such as establishing milk flow after a C/section, which has become a routine obstetric procedure, are hardly ever mentioned in literature. What’s more is that Izzy could afford the tools to help her lactate, and in many cases, women do not have the means to obtain such support. I also spoke with midwives who felt they didn’t receive enough training on how to support mothers who do not “take to the breast” for whatever reason (see also Dykes 2006).
By foregrounding some innate maternal capacity to breastfeed, public health literature overlooks that there is a generational gap of knowledge and practice. In the last decades, breastfeeding simply wasn’t trendy. The mother of Ava, one of my informants, was so disturbed by the sight of her lactating daughter that Ava decided not to involve her in any activities that would show her breastfeeding. To Ava’s mother, formula is an empowering solution that allowed her to go back to work and sustain the family. It is testimony to how little things have changed for Irish women since the 80s that for many, especially working-class parents, formula still presents a liberating and empowering tool. Women who do choose to breastfeed, require support. In Ireland, where women have been actively discouraged to breastfeed for decades before the introduction of a National Breastfeeding Policy, this support should be freely available from public health services, community centres and GPs.
When speaking of post-natal services, my informants had mixed feelings. When meeting a nurse or midwife who had experience with breastfeeding, they often found the support needed. Many also decided to avoid the public health nurse when they realised that they would be asked questions they could not answer. The charts and forms of post-natal check-ups are based on the reliability of formula’s calorific measurements. Parents simply couldn’t provide details to questions like, “How much are you feeding your baby?” or “How many feeds has baby had in the past 24 hours?” Some, like Karen, had their baby on the breast almost every hour during the first weeks, trying to calm the baby and feed it. The health charts do not function with such vague information. In fact, they do not account at all for breastfeeding as a practice that encapsulates more than just feeding. Growth charts require millilitres, times, intervals: the hard truths that leave the breastfeeding parent feeling insecure about their ability to care for their child. As such, formula may be more “natural” to Ireland than breast milk.
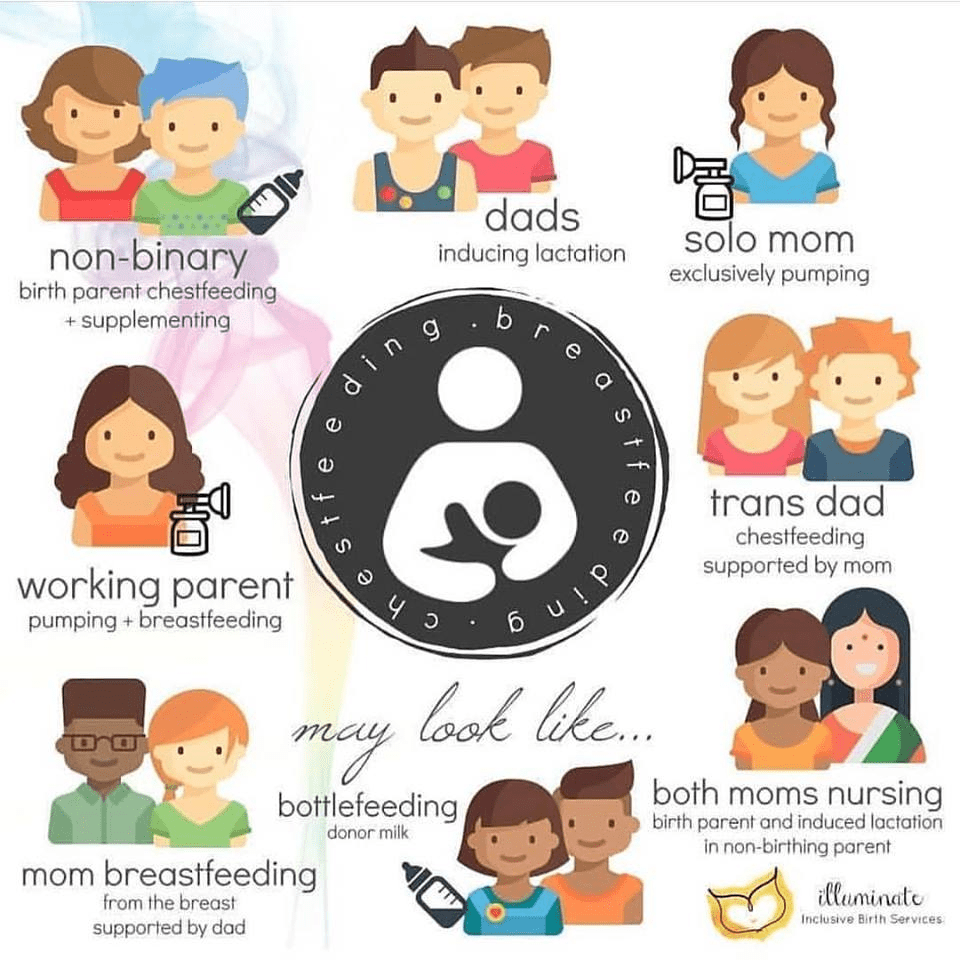
More than scientific rationales, and calls to “natural” motherhood, Irish mothers and parents who want to breastfeed anywhere need structural support, trained staff and time. Parental leave needs to be paid and take into consideration the needs of infants and parents alike. Medical staff need to be trained to encourage breastfeeding where it is wanted. In Ireland, parents must learn totally new skills and techniques to achieve this “natural” and particular form of child care. Breastfeeding is labour, and labour needs a union. This union is the support network made of parents, family, friends and health experts. I am convinced that it is neglectful to ask parents to take responsibility for breastfeeding and early childcare alone. Furthermore, the burden of care falls most heavily on people who lactate, especially for women in heterosexual relationships like my informants. A successful campaign should not stigmatise feeding decisions and prioritise the “natural” maternal capability to breastfeed but enable families of any shape to make a choice that suits their abilities.
If you would like to read more about breastfeeding and its politics, have a look at the suggested reading list.
Suggested Readings:
Kitzinger, S. (2005). The politics of birth. Edinburgh: Elsevier Butterworth Heinemann.
Koerber, A. (2013). Breast or bottle? Contemporary controversies in infant-feeding policy and practice. University of South Carolina Press.
Martucci, J. (2015). Back to the breast: Natural motherhood and breastfeeding in America. Chicago: The University of Chicago Press.
Williams, F. (2013). Breasts: A natural an unnatural history. W.W. Norton&Company.





Leave a comment