By: Giacomo Dentoni
What are the main challenges for low-income countries trying to achieve basic vaccination coverage? And what are the potential ramifications for their societies and economies? Giacomo Dentoni explores these questions in his article on COVID-19 vaccine inequity.
In most low-middle income countries (LMICs), less than 16% of adults are fully vaccinated against COVID-19. Now compare that to 72% in high income countries (HICs). Are lives in our countries more valuable than the ones in LMICs? Is it ethical to withhold lifesaving scientific discoveries from people that cannot afford them? Why is this vaccine being treated as a commodity rather than a lifesaving treatment for patients, communities, countries, and economies? Researchers, NGOs and activists are campaigning to change this absurd inequity, but governments and pharmaceutical companies are turning a deaf ear towards these pleas.
While vaccination campaigns in the Western world have made substantial progress, LMICs find themselves disadvantaged and left behind in the race against COVID-19. This inequity is clearly visualized in the map below where one can notice a low percentage of the population being vaccinated in some countries in South and South-East Asia, Latin America, the Middle East, and especially Africa. Countries such as Nigeria and Ethiopia, which make up 3% and 2% of the world’s population, vaccinated only 10.7% and 21% of their respective populations (accessed April 28th, 2022).

In African countries, the WHO target of achieving complete immunization cycle of 40% of the population by the end of December 2021 was missed. If things continue as they stand, the majority of African countries will only be able to complete their vaccination campaigns in 2023, two years behind most wealthier nations. The disparity in vaccine distribution has been dubbed the biggest failure of 2021 by World Health Organization Director General Dr. Tedros Adhanom Ghebreyesus.
As life slowly goes back to normal in HICs, with lockdowns and restrictions easing as well as effective inoculation campaigns underway, there seems to be an overwhelming misconception that we have reached the end stages of the pandemic. Fourth doses are being offered in some countries to elderly and immunosuppressed patients. Will the adult population soon follow suit? Although waning immunity has been used as an argument for the need of further inoculations (see also), death or hospitalizations remain extremely rare in healthy fully vaccinated individuals after the third COVID-19 dose. WHO guidelines for booster doses state that offering follow-up vaccinations to the healthy population needs to be firmly evidence-driven and targeted to the population groups in greatest need. Giving boosters in highly immunized populations effectively means taking vaccines away from the 2.8 billion people who have not yet received any.
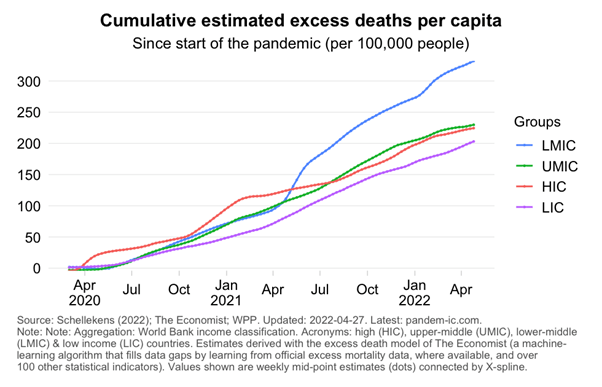
Why is basic protection against COVID-19 not being granted to the Global South? Why are healthcare workers, the elderly, and vulnerable populations in LMICs being excluded, while the entire adult population in HICs is offered booster doses? Vaccine hoarding has often been justified by the Global North due to being hit harder by the pandemic as a result of their ageing population. However, recent estimations of excess death during the COVID-19 pandemic shows that LMICs (blue line in graph below) have had the highest cumulative excess mortality rates since June 2021, likely due to direct (LMICs’ delayed vaccination campaigns and minimal capacity to deal with severe COVID-19 cases) and indirect effects (disruption of health systems and decreased access to food) of the COVID-19 pandemic.
Furthermore, limited vaccination coverage means that the virus finds a perfect breeding ground, and the likelihood of more dangerous vaccine-resistant variants emerging increases, which we experienced in southern Africa with the Omicron variant at the end of 2021. A pre-print predicted such a scenario, reporting that vaccination coverage rate is inversely correlated to the mutation frequency of COVID-19 delta variants (see Figure 1,A) . Countries with low vaccination coverage such as India report increased mutation frequency, while on the other hand Israel that vaccinated most of its population quite early on into the pandemic, records low mutation incidence.
On top of these issues, various logistical barriers prevent equitable vaccine distribution in LMICs. These include lack of investment to strategically deliver vaccines, maintaining cold chain distribution, lack of vaccine manufacturing capacity, and prices of certain vaccine manufacturers being bought by LMICs at higher prices compared to HICs. With COVID-19 expenditure piling up and recurring outbreaks in LMICs, the situation could lead to substantial economic losses and fragile economies having to increasingly depend on international loans. Countries in the Global South will be forced to cut back on development plans, leading to setbacks in some of the Sustainable Development Goals (SDGs) targets. Indeed, disruption in healthcare services due to COVID-19 can have a ripple effect on other vital services such as HIV treatment and childhood immunisation campaigns in countries where healthcare resources are already scarce and with complex political situations.
To address vaccine inequity on a global scale, the COVAX initiative (co-managed by CEPI, Gavi and WHO, together with delivery partner UNICEF) was launched in the summer of 2020, aiming to guarantee fair and equitable access to COVID-19 vaccines for every country, regardless of income. Thanks to COVAX, around 1.5 billion doses have been delivered to the world’s poorest economies.
As citizens of wealthier nations whose multiple vaccinations were covered by the national healthcare, it is our responsibility to put pressure on our politicians to stand by their words and provide continued support for LMICs with doses pledged. “No one is safe until everyone is safe” unless barriers for vaccine delivery are eliminated and pressure to lower vaccine prices for LMICs is put on pharmaceutical companies, which have emerged from the pandemic exponentially richer. On a smaller scale, there are ways to contribute. For 10$, one dose can reach a country in need through direct donations to the COVAX initiative set up by Vaccine Forward (QR code below).
Ending COVID-19 must remain high in the political agenda, together with important societal and political events including the war in Ukraine, the energy crisis, and a looming global recession. Global inequities in access to vaccines will persist unless we take action now to ensure a fair and transparent global allocation of lifesaving resources for the current outbreak and fair distribution for future pandemics.





Leave a comment